HERO Reviewer:
Gregg M. Gascon, PhD, Advanced Analytics Consultant, Ohio State University Health Plan
This industry research review departs from past practice by examining two studies rather than one. This approach is appropriate in the current context due to the nature of the focal study: a systematic review of workplace interventions for reducing sitting at work. As will be seen shortly, the research question explored by the Cochrane Collaboration Work Group is narrow, which is appropriate to the research methodology. However, to appreciate where the study results fit into the wider body of research into workplace interventions to lower health risks, a second study augments the perspective of the first in order to edify the research review.
Study Citations:
Shrestha N, Kukkonen-Harjula KT, Verbeek JH, Ijaz S, Hermans V, Bhaumik S. Workplace interventions for reducing sitting at work. Cochrane Database of Systematic Reviews. 2016; 3: CD010912.
Angadi SS, Weltman A, Watson-Winfield D, Weltman J, Frick K, Patrie J & Gaesser GA. Effect of fractionized vs continuous, single-session exercise on blood pressure in adults. Journal of Human Hypertension. 2010; 24(4):300-302.
Study Overview: Cochrane Study
For a number of decades, the proportion of American workers who are physically active at the worksite has steadily declined. The number of studies reporting negative correlations between physical activity and rates of cardiovascular disease, obesity, diabetes and mortality have risen at the same time. In response, employers have sought a variety of ways to increase workplace physical activity in order to reduce morbidity and mortality. The Cochrane Collaboration recently reviewed the evidence behind the effectiveness of such workplace interventions.
The Cochrane Collaboration (http://www.cochrane.org/) is an international organization of health care practitioners and researchers whose primary aim is to support evidence-based decision making by preparing, maintaining and promoting the accessibility of systematic reviews of the evidence for the prevention and treatment of specific health problems. Its work is supported by 53 review groups that are responsible for preparing and maintaining reviews within specific health care areas. The Work Group recently released its updated evidence guidance on workplace interventions for reducing sitting time at work.
The basis of Cochrane Collaboration work is the systematic review. A systematic review represents a vigourous attempt to aggregate all empirical evidence that fits pre-specified eligibility criteria in order to answer a specific research question. This methodology is published as a protocol prior to conducting the research in order to reduce the impact of review authors’ biases, produce transparency, reduce the potential for duplication, and allow peer review of the planned methods (Light, 1984). Once the review is complete, the research is updated every two years as necessary; if no update is required, a commentary is published by the authors to explain their reasoning. This allows each review to provide the best available empirical research on the subject to be quickly available to the public.
Cochrane Study Results
The updated systematic review ‘Workplace Interventions for Reducing Sitting at Work’ was released March 17, 2016. The original protocol was released in 2014; the first update was published in 2015. The original protocol limited studies to the following:
- Randomized controlled trials (RCTs);
- Cluster RCTs and quasi-RCTs (trials that intend to randomize participants to the intervention or control group but where the method of randomization is not random);
- Adults aged 18 years and above whose occupations involve the majority of working time sitting at a desk, such as in administrative jobs, customer service, help desk professionals, call center representatives and receptionists; and
- Three types of interventions: physical changes in workplace environment, a policy to change the organization of work, or information and counselling to encourage workers to sit less.
Two types of outcome measures were to be assessed in the review: primary (self-reported time spent seated at work by various questionnaires or objectively measured sitting by means of an inclinometer which assesses body posture); and secondary outcomes (energy expenditure measured in METs hours per work day as a proxy measure for reduction in sitting; changes in productivity; and adverse events including any reported musculoskeletal symptoms or varicose veins due to prolonged standing).
The updated systematic review published in 2016 included 20 studies, of which 11 were controlled trials. The studies included physical workplace changes (sit-stand desks, treadmill desks and pedaling workstations), policy changes regarding walking, information and counselling (counselling, mindfulness training, computer prompting) and interventions from multiple categories. The authors found very low to low quality evidence that sit-stand desks decrease workplace sitting between 30 minutes to 2 hours per day without having adverse effects in the short- or medium term (and no long-term evidence), and no considerable or inconsistent effects of other interventions such as policies or information and counselling. Thus, the Cochrane Work Group concluded there was very low to low quality evidence that sit-stand desks or related interventions could prevent the harm associated with prolonged sitting at work, and no evidence of an effect in the long term. The Work Group suggested that researchers design large-scale randomized studies with adequate sample sizes and long-term follow up to test the effects of such interventions on reducing sitting time at work.
Reviewer Commentary
While the systematic review targeted studies that were developed and implemented in order to reduce sitting time at work, the larger question is what employers and employees can do together in the workplace to reduce the risk of chronic disease. Thankfully, there is evidence from a series of studies that highlight interventions that are impactful for health improvement and respectful of work responsibilities.
Cardiovascular (heart) disease is the number one cause of death among Americans (National Center for Health Statistics, 2015). One of the strongest risk factors for cardiovascular disease is blood pressure levels (MacMahon, 1990). Researchers have conducted multiple trials to identify interventions to lower blood pressure among persons at each blood pressure level that can be easily implemented in the workplace.
One seminal study (Angadi et al, 2010) examined the impact of three, 10-minute walks per day on blood pressure levels. In the study, 29 sedentary, healthy men and women refrained from exercise 24 hours prior to the study. They were admitted to a research center the night before the study, where they ate standardized meals the evening before the study. The following morning, participants were randomly assigned to either one 30-minute or three 10-minute exercise sessions on a treadmill. Thereafter, the participants rested. The following day all participants rested. Blood pressure was measured hourly from 0900 – 2100 by research center nurses blinded to the experimental treatment condition.
Compared with both control and the 1 X 30-minute exercise conditions, systolic blood pressure was lower hour by hour (Figure a) and in the aggregate (Figure b) under the 3 X 10-minute exercise condition. Thus, fractionized exercise spaced evenly throughout the day was superior to either comparison for lowerering systolic blood pressure in the afternoon and early evening hours.
Figure: Pattern of SBP across 24 h comparing 3 X 10-min and control conditions
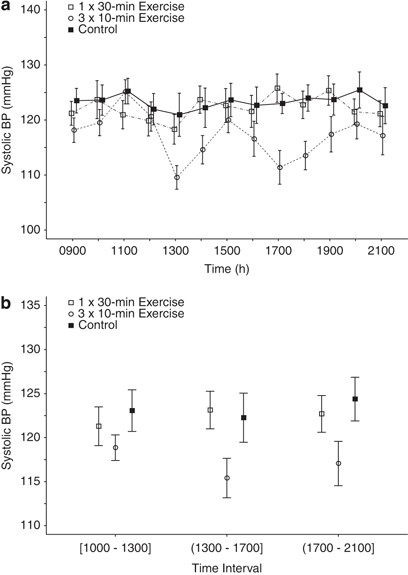
(a) Hourly BPs for each condition. (b) Four-hour aggregate systolic BP (SBP) during the control day, a day in which a single, continuous 30-min exercise session was performed (0900–0930 hours), and on a day in which three 10-min exercise sessions were performed (0920–0930; 1320–1330; 1720–1730 hours). Values are mean ± s.e.m. and represent data from all subjects (n = 29) combined. SBP was significantly lower during 3 × 10 min compared with the other two conditions at >1300 through 1700 hours (p = 0.013 vs control; p = 0.004 vs 1 × 30 min) and >1700 through 2100 hours (p = 0.020 vs control; p = 0.018 vs 1 × 30 min).
Like all good scientific studies, these results represent one link in a long chain of studies that occurred before and after this study. These results extended the findings of previous research that found fractionized exercise to be superior to a single continuous exercise session in prehypertensives (Park, Rink & Wallace, 2006) to normotensive individuals. It also led to studies that unpacked the differences between walking, standing and cycling on blood pressure (Zeigler et al., 2015) and led to exercise recommendations for patients with hypertension (Pescatello et al., 2015).
A wealth of evidence exists that demonstrates the positive impact of exercise on healthy and unhealthy individuals (see, for example, Haskell et al., 2007). However, many do not pursue exercise because of time constraints. What the Angadi et al. study adds to that literature base is that cardiovascular health risks can be reduced with as little as three 10-minute walks a day. This type of exercise regimen can be implemented in nearly every American workplace without disruption, without additional employer costs, and with minimal employee investment. The benefits of this intervention are enormous: “Even if the average SBP reduction was just 5 mm Hg, if achieved daily, it could potentially reduce stroke incidence by 14%, cardiovascular mortality by ~ 9%, and overall mortality by 7%” (Whelton et al., 2002, as cited in Angadi et al., 2010, 302).
The Health Enhancement Research Organization has also completed a number of research studies to improve health at the workplace; many are available at https://hero-health.org/research/hero-research-studies. While some review interventions designed to decrease morbidity, others explore ways in which to measure health and health outcomes at work. These studies complement a rich literature on the subject including Pronk (2009), O’Donnell (2014) and Hanson (2007).
About the HERO Reviewer
Gregg M. Gascon, PhD
Dr. Gascon, Director, Advanced Analytics Consultant, serves as a member of The Ohio State University Health Plan (OSUHP) senior operations team. He coordinates health and wellness research in support of the University’s Office of Human Resources’ benefits programming, the University’s Chief Wellness Officer, and the One University Health and Wellness Council. He also works with the College of Medicine and Public Health in support of OSUHP and the University’s population health management strategy. As principal investigator for OSUHP, he works with University and Medical Center faculty to develop solutions to address the rate of increase in treatment costs of the University’s benefits program, and builds internal expertise and research capabilities to support growth initiatives. OSUHP administers health insurance benefits to over 63,000 employees and dependents of the University and Medical Center, and provides wellness services to community employers. In the interests of full disclosure, Dr. Gascon is a a member of the Cochrane Methodology Review and Work Groups.
References
Angadi SS, Weltman A, Watson-Winfield D, Weltman J, Frick K, Patrie J, & Gaesser GA. Effect of fractionized vs continuous, single-session exercise on blood pressure in adults. Journal of Human Hypertension. 2010; 24(4): 300-302.
Hanson A. Workplace health promotion: a salutogenic approach. 2007. Bloomington, IN: AuthorHouse.
Light RJ & Pillemer DB. Summing up: The science of reviewing research. 1984. Cambridge, MA: Harvard University Press.
MacMahon S, Peto R, Collins R, Godwin J, Cutler J, Sorlie P, et al. Blood pressure, strike, and coronary heart disease: part 1, prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. The Lancet. 1990; 335(8692): 765-774.
National Center for Health Statistics. Health, United States, 2014: With special feature on adults aged 55-64. 2015. Washington, D.C.: U.S. Government Printing Office.
National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2004; 42:1206–1252.
O’Donnell MP. Health promotion in the workplace: Improving awareness, enhancing motivation, building skills and creating opportunities (4th Ed.). 2014. CreateSpace Independent Publishing Platform.
Park S, Rink LD & Wallace JP. Accumulation of physical activity leads to a greater blood pressure reduction than a single continuous session, in prehypertension. Journal of Hypertension, 2006; 24(9):1761-1770.
Pescatello LS, MacDonald HV, Ash GI, Lamberti LM, Farquhar WB, Arena R & Johnson BT. Assessing the existing professional exercise recommendations for hypertension: a review and recommendations for future research priorities. Mayo Clinic Proceedings. 2015: 90(6):801-812.
Pronk NP (Ed). ACSM’s worksite health handbook: A guide to building healthy and productive companies (2nd Ed.). 2009. Champaign, IL: Human Kinetics.
Shrestha N, Ijaz S, Kukkonen-Harjula KT, Kumar S, Nwankwo CP. Workplace interventions for reducing sitting at work (Protocol). Cochrane Database of Systematic Reviews. 2014; 1:CD010912.
Shrestha N, Ijaz S, Kukkonen-Harjula KT, Kumar S, Nwankwo CP. Workplace interventions for reducing sitting at work. Cochrane Database of Systematic Reviews. 2015; 1:CD010912.
Shrestha N, Kukkonen-Harjula KT, Verbeek JH, Ijaz S, Hermans V, Bhaumik S. Workplace interventions for reducing sitting at work. Cochrane Database of Systematic Reviews. 2016; 3:CD010912.
Whelton PK, He J, Appel LJ, Cutler JA, Havas S, Kotchen TA, et al. Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program. Journal of the American Medical Association. 2002; 288(15): 1882-1888.
Zeigler ZS, Mullane S, Crespo NC, Buman MP & Gaesser GA. Effects of standing and light-intensity activity on ambulatory blood pressure. Medicine and Science in Sports and Exercise. 2015; 48(2):175-81.