 Zaira Chaudhry, MD, MPH worked with HERO as a Research Intern from January – May 2020. She is a physician-in-training who earned her M.D. at the Geisinger Commonwealth School of Medicine. She also holds an MPH from the University of New England and a B.S. in Human Biology from Cornell University. Throughout her medical training, Zaira has engaged in research efforts to advance the practice of clinical medicine. She is particularly interested in occupational and environmental medicine. Zaira is passionate about promoting workplace health and wellness and hopes to leverage her background in medicine and public health to contribute to the field.
Zaira Chaudhry, MD, MPH worked with HERO as a Research Intern from January – May 2020. She is a physician-in-training who earned her M.D. at the Geisinger Commonwealth School of Medicine. She also holds an MPH from the University of New England and a B.S. in Human Biology from Cornell University. Throughout her medical training, Zaira has engaged in research efforts to advance the practice of clinical medicine. She is particularly interested in occupational and environmental medicine. Zaira is passionate about promoting workplace health and wellness and hopes to leverage her background in medicine and public health to contribute to the field.
Introduction
Illness or injury may potentially result in temporary or permanent disability, which encompasses impairments, activity limitations, and participation restrictions that can have significant implications for both employees and their employers.1 In 2016, approximately 11% of U.S. adults between the working-ages of 18 and 64 had a disability, and it is estimated that nearly 6% of employed individuals in the United States experience a short-term disability each year.2,3 Therefore, it is imperative that employers have an understanding of the regulatory environment surrounding employee disability and best practices for disability management (DM), which serves to minimize the disabling impact of illnesses and injuries that develop during the course of employment and maximize the employee’s ability to participate in the work environment.
This commentary explores DM initiatives among employers who have completed the HERO Health and Well-being Best Practices Scorecard in Collaboration with Mercer© (HERO Scorecard), which includes several questions related to DM initiatives, as noted below. An analysis was performed using data from the HERO Scorecard Benchmark Database to understand the state of DM among 1,199 unique organizations who completed the relevant sections of the HERO Scorecard as of December 31, 2019. In addition to assessing how employers are supporting DM and its integration with health and well-being (HWB) initiatives within their organizations, this commentary also explores whether disability practices differ by employer size.
Prevalence of Disability Management Practices
Of the 1,199 organizations that completed the HERO Scorecard, 916 (76%) organizations reported using at least one DM practice listed in the scorecard, although the prevalence of each practice varied considerably. The remaining 283 (24%) organizations have not implemented any of the DM practices discussed below, with 142 of these organizations being small employers (< 500 employees).
Only 13% of organizations have formal goals for their disability programs, and 9% of organizations have performance standards to hold leaders, managers, and supervisors accountable for these goals. Approximately half (52%) of the organizations have written return-to-work programs with policies and procedures covering all absences, and 44% of organizations have established standards for ongoing communication with employees during the duration of their leave. Fifty-seven percent (57%) of organizations have modified temporary job offers for employees with disabilities who are ready to return to productive activity but not to their former jobs. In 34% of the organizations, complex claims receive clinical intervention or oversight by in-house or outsourced staff. Only 18% of organizations have developed metrics to regularly monitor/manage disability trends. Fourteen percent (14%) of employers use strategies to triage individuals with certain disabilities into relevant employee health management programs.
In terms of DM program integration with HWB initiatives, 19% of organizations have a process for referring employees in their DM program to health management programs. Moreover, 9% of organizations combine disability data with health management program data for identifying, reporting, and performing analytics. Only 2% of organizations offer a more generous disability benefit to employees who participate in appropriate health management programs. However, the majority (76%) of organizations do not integrate their DM programs with HWB initiatives as described above.
Disability Management Practices by Employer Size
For this analysis, organizations were categorized into three distinct groups based on their self-reported number of employees. The groupings were consistent with prior HERO Scorecard benchmark reports. “Small” organizations were those that reported having less than 500 employees. “Mid-size” organizations were those that reported having between 500 and 4,999 employees. “Large” organizations were those that reported having 5,000 or more employees.
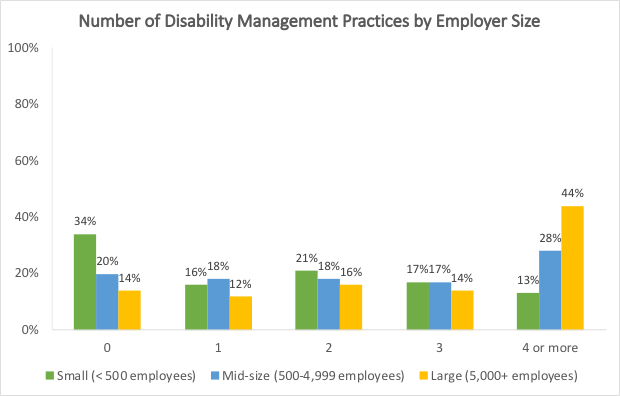
The prevalence of each DM practice was highest among large organizations, followed by mid-size organizations, and lowest among small organizations. Moreover, the number of DM practices varied according to employer size, with large organizations implementing more practices than mid-size and small organizations as noted below and in Figure 1:
- 0 practices: 34% of small organizations, 20% of mid-size organizations, 14% of large organizations
- 1 practice: 16% of small organizations, 18% of mid-size organizations, 12% of large organizations
- 2 practices: 21% of small organizations, 18% of mid-size organizations, 16% of large organizations
- 3 practices: 17% of small organizations, 17% of mid-size organizations, 14% of large organizations
- 4 or more practices: 13% of small organizations, 28% of mid-size organizations, 44% of large organizations
Figure 1. Number of disability management practices by employer size
Among small organizations that implemented one or more DM practices, the most frequently implemented practices were modified temporary job offers for employees with disabilities who are ready to return to productive activity but not to their former jobs (76% vs. 75% of larger employers), written return-to-work programs with policies and procedures covering all absences (65% vs. 69% of larger employers), and standards for ongoing supportive communication with employees throughout the duration of their leave (59% vs. 56% of larger employers).
A similar trend based on employer size was noted with respect to DM program integration with HWB initiatives, although the prevalence of integration practices was surprisingly low among all organizations. Over a quarter (29%) of large employers have a process for referring employees in DM programs to HWB programs, whereas only 13% of small organizations and 19% of mid-size organizations implemented this practice. Likewise, large organizations were more likely to combine disability data with HWB program data for identifying, reporting, and performing analytics than mid-size and small organizations (15%, 9% and 4%, respectively).
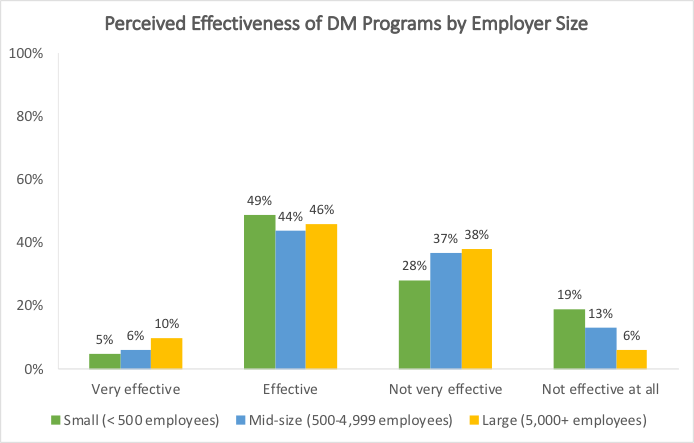
When asked about their opinions regarding the effectiveness of their DM programs in promoting a healthier, more productive workforce, nearly 50% of employers, regardless of size, considered their DM initiatives to be “effective” as noted below and in Figure 2:
- Very effective: 5% of small organizations, 6% of mid-size organizations, 10% of large organizations
- Effective: 49% of small organizations, 44% of mid-size organizations, 46% of large organizations
- Not very effective: 28% of small organizations, 37% of mid-size organizations, 38% of large organizations
- Not effective at all: 19% of small organizations, 13% of mid-size organizations, 6% of large organizations
Figure 2. Perceived effectiveness of disability management programs by employer size
Discussion and Conclusions
These findings indicate that there is considerable variability in the adoption of different practices to support DM among employers, with relatively few organizations taking measures to integrate their DM programs with employee HWB initiatives despite the increased focus on moving away from fragmented approaches for promoting employee safety and wellness and toward a more integrated approach in recent years.4
According to prior research, employer support and ongoing communication with employees during leave due to illness or injury may influence employees’ attitudes toward the return-to-work process.5 Therefore, more organizations may want to consider establishing standards for ongoing communication as part of their DM initiatives and ensure appropriate training for supervisors to effectively support the return-to-work process. More organizations may also want to consider offering opportunities for transitional duty or modified work to employees with disabilities who are ready to return to productive activity but not to their former jobs, as there is evidence suggesting that this practice may promote earlier return-to-work, which benefits both the employee and employer.6
From a practical standpoint, it makes intuitive sense that larger organizations generally employ a more robust approach to DM as evidenced by the findings presented above. While it is possible that a more comprehensive approach to DM is beneficial for both employees and employers, such an approach likely requires additional resources that smaller organizations may lack. Employers’ perceived program effectiveness does not appear to differ drastically between organizations of different sizes.
Further research in this area may be of interest to employers, particularly research that addresses whether the implementation of more DM practices translates to increased rates of return-to-work and/or reductions in time to return-to-work following the onset of disability.
HERO would like to thank and acknowledge the following HERO Scorecard commentary reviewers: David Anderson (VisioNEXT, LLC), Kerry Evers (Pro-Change Behavior Systems), Stefan Gingerich (StayWell/WebMD Health Services), Jessica Grossmeier (HERO), Mary Imboden (HERO), and Steven Noeldner (Mercer).
References
- World Health Organization (WHO). Disabilities [webpage]. Available at: https://www.who.int/topics/disabilities/en/. Accessed Feb 10, 2020.
- Kraus L, Lauer E, Coleman R, Houtenville A. 2017 Disability Statistics Annual Report. Durham, NH: University of New Hampshire. Available at: https://disabilitycompendium.org/sites/default/files/user-uploads/2017_AnnualReport_2017_FINAL.pdf. Accessed Feb 10, 2020.
- Integrated Benefits Institute, Health and Productivity Benchmarking 2016 (released November 2017), Short-Term Disability, All Employers. Group average for new claims per 100 covered lives. Available at: https://www.ibiweb.org/benchmarking/. Accessed Feb 10, 2020.
- Schill AL, Chosewood LC. The NIOSH Total Worker Health™ program: an overview. J Occup Environ Med. 2013 Dec;55(12 Suppl): S8-11.
- Buys NJ, Selander J, Sun J. Employee experience of workplace supervisor contact and support during long-term sickness absence. Disabil Rehabil. 2019 Apr;41(7): 808-814.
- Shaw WS, Nelson CC, Woiszwillo MJ, Gaines B, Peters SE. Early return to work has benefits for relief of back pain and functional recovery after controlling for multiple confounds. J Occup Environ Med. 2018 Oct; 60(10): 901–910.
{kind=link}