
Tatiana Shnaiden, MD MS
By Tatiana Shnaiden, MD MS
Dr. Tatiana Shnaiden is a Health Analytics leader, and her specialty is science and analytic support for improving health and quality of care for a population at an affordable cost. She has built and managed health analytic functions for health plan, clinical decision support, care management and employee benefit areas, translating data and information into actionable insights for population health stakeholders while employing wide range of data analytic methods from descriptive to predictive and prescriptive models. Dr. Shnaiden graduated from Russian State Medical University and received her MS in Biostatistics from New York Medical College.
The latest advancements in data collection, management and analytic technologies have created an opportunity for the health promotion field to move towards more informed decision-making by using various data to effectively measure and manage the health and well-being (HWB) of the population. In addition, using the HERO Health and Well-Being Best Practices Scorecard in Collaboration with Mercer© (HERO Scorecard) as a tool to establish measurements and to benchmark them against other organizations, the Scorecard also collects information on the use of data in population HWB improvement.
Data from the HERO Scorecard Benchmark Database was used to understand the state of informed decision making in HWB among 1,056 organizations who completed the HERO Scorecard as of December 31, 2018. Only half of the organizations responding to the HERO Scorecard (50%) perceive that their data management and evaluation activities effectively or very effectively contribute to the success of their organization’s HWB initiative. For more insights on this issue we looked at the organizations’ perception of the effectiveness of their organizational support strategies in promoting the HWB of employees; the data types they use to assess individual or population health; the data being used to evaluate and manage the HWB program, and the stakeholders who regularly receive HWB program performance data and information. We also explored the connections between using data and information for assessing the health of the population and perceptions about program effectiveness, as well as how communication of program performance to various stakeholders relates to the use of data for assessing the health of the population and program effectiveness. Further analysis examines whether organizations that report having effective organizational support practices are more likely to use data to assess the health of their population, communicate program performance to stakeholders, and use data to evaluate their HWB initiatives.
Results
Among various data sources for assessing the health of the population, health assessment is used by 66% of the 1,049 employers, biometrics by 64%, and medical claims by 61%. A surprising number of organizations (12%) report not assessing the health of their population. The three data types most commonly used to evaluate and manage HWB initiatives are program participation data (used by 73% of HERO scorecard completers), population physical health risk data (48%), and healthcare utilization/cost data (55%). Fourteen percent (14%) of employers do not use any data to evaluate and manage HWB initiatives. Most frequently reported recipients of program performance information are senior leaders (59%). Employers are less likely to share program performance data with managers (24%), employees (22%), or vendors (20%). One third (33%) of the organizations do not share HWB program performance data with any stakeholders.
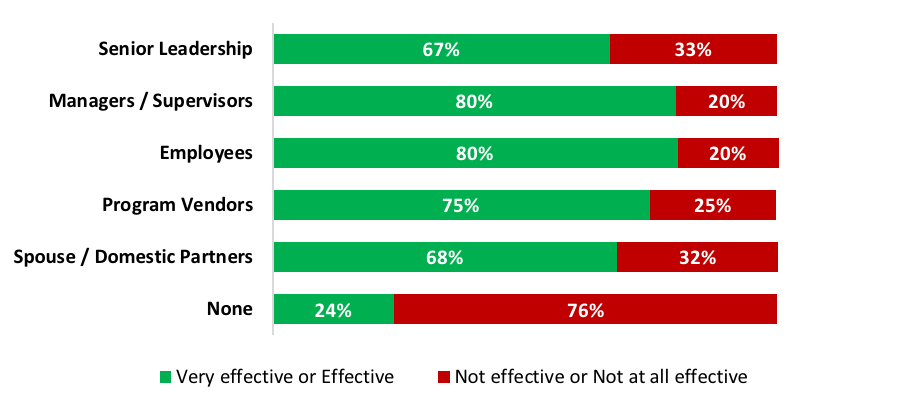
Organizations that collect and use at least one source of data are more likely to view their organizational support strategies as effective. Conversely, 84% of the organizations that do not capture any data to evaluate and manage their HWB programs report their organizational support strategies are “not effective/not at all effective” (see figure 1). A majority (76%) of those that do not share data with any stakeholders report that their organizational support strategies as “not effective/not at all effective” (see figure 2). In contrast, 67% of the organizations that regularly share HWB program performance data with senior leadership report that their organizational support strategies are effective or very effective.
Figure 1. Subjective effectiveness rating based on use of data for program evaluation
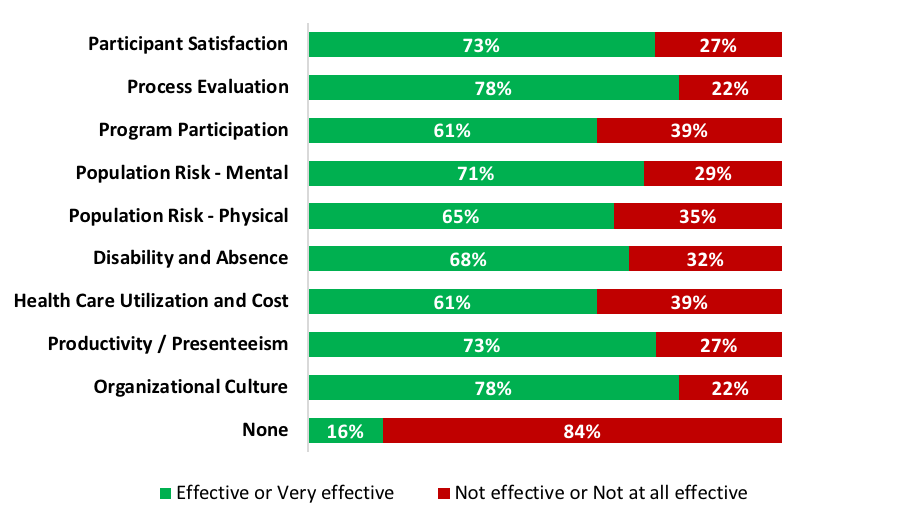
Figure 2. Subjective effectiveness rating based on sharing data with stakeholders
Among organizations reporting that their organizational support strategies on HWB are effective, the most used data sources are program participation data (84%), health utilization and cost data (62%), and participant satisfaction data (60%). Employers that report their HWB strategies to be effective or very effective are more likely to share program performance data with at least one stakeholder group (85% vs 48% for employers that report their HWB strategies not effective or not at all effective). Of the stakeholders reported to receive program performance data, 73% are senior leadership, 33% are managers/supervisors, 31% are employees, and 29% are program vendors. The types of data these organizations most commonly used to evaluate program performance and share with stakeholders are health assessment (79% to 85%), biometric screening (76% to 80%) and claims data (74% to 80%). Virtually all (99%) of the organizations reporting their HWB initiatives as very effective use at least one data type for evaluation and management.
Discussion
This analysis clearly indicates that there are opportunities for improvements in the use of data, since 12% of organizations do not use any data in assessing the health of their population and 14% do not use data for program evaluation and management. Lack of data utilization is connected to a higher likelihood that the HWB initiative is perceived to be ineffective.
Sharing of HWB results with senior leaders seems to be a strong driver of whether data are used for program evaluation. However, there is a significant gap between the percentage of organizations that share performance results with senior leadership (59%) versus with managers/supervisors (24%). Given the important role middle managers and front-line managers play in HWB program success,1,2 organizations aiming to improve the effectiveness of their HWB initiatives should regularly share program results with managers and supervisors. Organizations that do not perceive their HWB initiatives as effective may be able to improve outcomes by sharing their HWB results with stakeholders to identify opportunities for possible course corrections and set realistic expectations for future outcomes. Some health promotion professionals may be reluctant to share negative program performance results with stakeholders, particularly with senior leadership. Nevertheless, sharing program performance data, whether results are positive or negative, creates accountability and provides an opportunity to get more stakeholders engaged in opportunities to improve a HWB initiative over time through continuous learning and quality improvement.
Organizations that use data to evaluate HWB program performance are more likely to report that the HWB initiative is effective compared to those that do not use data to evaluate their program. It is likely that sharing evidence of program performance helps build confidence that program offerings are directly connected to employee health improvement outcomes. Furthermore, organizations with stronger performing programs may be more likely to invest in robust data collection and reporting.
Implications for Practice
This analysis offers at least three process improvement ideas for health promotion professionals. First, the fact that 33% of organizations do not share data with any stakeholders indicates there are significant opportunities to incorporate use of data to enable more participative decision making in designing HWB initiatives. Second, use of data to measure and evaluate HWB initiatives may influence perceptions of program effectiveness. While measurement and evaluation efforts may not always yield favorable results, framed properly they should produce actionable insights that can be used to improve initiative performance. Third, HWB program strategists have an opportunity to gain support from senior leadership to invest in data collection and to make program performance results more transparent to middle management and front-line supervisors, which may engage many more stakeholders in supporting HWB efforts.
This commentary is based on data from the HERO Scorecard Benchmark Database through December 31, 2018.
References
- HERO Scorecard Health and Well-being Best Practices Scorecard in Collaboration with Mercer. HERO Scorecard Benchmark Database through December 31, 2018.
- Zahrt O. Leadership Support and the Effectiveness of Wellness Initiatives. HERO Health and Well-being Best Practices Scorecard in Collaboration with Mercer 2018 Progress Report. 2018: 30-33.
- Hamill L. Organizational Support for Well-being Senior Leadership and Managerial Support Required. HERO Health and Well-being Best Practices Scorecard in Collaboration with Mercer 2018 Progress Report. 2018: 36-39.
{kind=link}